Neonatal Cooling Device for Hypoxic-Ischemic Encephalopathy (Asphyxia)
Neonatal Cooling Device:
The neonatal cooling device is used to reduce and treat brain injuries and neurological dysfunctions caused by asphyxia in newborns. When encephalopathy in a newborn occurs due to reduced oxygenation of the blood (hypoxia) and decreased blood flow (ischemia) in the brain, it is referred to as hypoxic-ischemic encephalopathy or asphyxia. This condition can have maternal, fetal, or placental origins. During hypoxic-ischemic brain injury, three phases of brain cell damage or death occur. The initial phase causes necrotic damage and brain cell death shortly after the onset of asphyxia. The latent phase occurs 2-8 hours after the hypoxic-ischemic injury, providing an opportunity for specific treatments like cooling therapy to prevent further brain damage. The secondary phase of injury starts 6-24 hours after the injury and can continue for several days. The tertiary phase can last from weeks to years after the initial injury.
The only known and approved treatment that can reduce the severity of moderate or severe encephalopathy is head or whole-body therapeutic hypothermia. This method is performed as a specific treatment protocol with defined inclusion and exclusion criteria. In the standard cooling therapy plan, treatment must begin within the window from birth to a maximum of 6 hours after birth, and the core body temperature should be lowered to 33.5 ± 0.5 degrees Celsius. The temperature is then maintained in this range for three days (72 hours). Afterward, the body is gradually warmed to normal temperature at a rate of 0.5 degrees Celsius per hour.

Components and Functions of the Device:
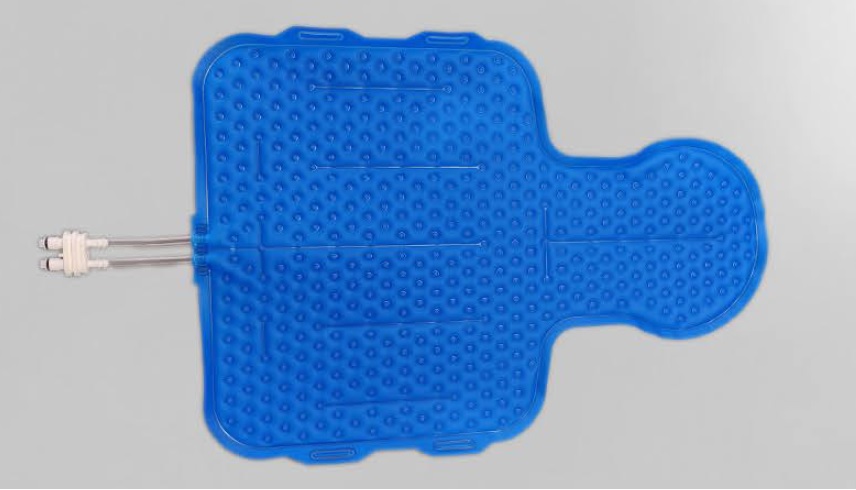
The device consists of three main parts: the main unit, the cooling mattress, and auxiliary equipment including connecting tubes for the coolant and skin and rectal sensors. In this device, distilled water is used as the coolant, which is chilled by a thermoelectric cooling system and transferred to the mattress through the connecting tubes. The mattress is soft, flexible, and made of polyurethane, placed under and wrapped around the newborn. As the coolant circulates through the mattress, the newborn’s body temperature decreases.
Cooling Therapy Mode Based on Standard Treatment Protocol
Multi-Point Temperature Control Mode
This mode is designed based on the standard treatment protocol for asphyxia. When activated, the cooling process for the newborn begins as quickly as possible. According to the cooling therapy protocol, the newborn’s rectal temperature, as an indicator of core temperature, is continuously monitored throughout the treatment. Cooling continues until the rectal temperature reaches 33.5 degrees Celsius. From this point, the temperature is maintained at this level for 72 hours based on rectal temperature readings and controller performance. After this period, the electric heating system activates, gradually increasing the newborn’s temperature at a rate of 0.5 degrees Celsius per hour until it reaches 37 degrees Celsius. The functional parameters of this temperature scenario include about 20 parameters, which the user can adjust based on the neonatologist’s discretion, using either default settings or other configurations.
Temperature Management Modefor Use as a Warmer or Normal Temperature
Stabilizer Single Point Temperature Control Mode In addition to the cooling therapy mode based on the standard treatment protocol, this device also has a temperature management mode for use as a warmer or normal temperature stabilizer. In this mode, the target rectal temperature is set by the user, and the device automatically performs cooling or heating operations at the set rate or maximum capacity until the target temperature is reached, then maintains the newborn’s temperature within this range with minimal fluctuations. This mode effectively transforms the device into a temperature stabilization system for hypothermia, hyperthermia, or normothermia treatments.
Technology Level
Currently, cooling therapy is performed using two methods: passive and active. In passive cooling therapy, the infant’s temperature is lowered by reducing clothing and ambient temperature, and using fans and ice packs. In this method, the core temperature must be monitored by measuring rectal temperature every 15 minutes by the NICU nurse. Clearly, this method lacks precision and effectiveness. However, in active cooling therapy, the infant’s temperature is reduced through contact with a cooling mattress, and the core temperature is continuously monitored and the mattress temperature adjusted to maintain 33.5 degrees Celsius for 72 hours. This method is highly accurate and effective; in 2010, the International Liaison Committee on Resuscitation (ILCOR) and the American Heart Association recommended that infants with moderate or severe encephalopathy diagnosed within the first 6 hours of life should receive this treatment. When this company began manufacturing the device, only three companies worldwide (from the UK, Israel, and the USA) were producing it, and only the UK model had been imported due to sanctions by other companies. The high cost of the UK model, along with the lack of official imports and effective support for maintenance and repairs, has resulted in the absence of active cooling therapy equipment in most NICUs in the country.
Prevalence of Hypoxic-Ischemic Encephalopathy (HIE)
The prevalence of this condition in developed countries is between 1 to 3 cases per 1,000 live births, whereas in low- and middle-income countries, it ranges from 7 to 20 cases per 1,000 live births, causing the death of 840,000 newborns annually worldwide. Without treatment, 62% of infants with brain damage due to perinatal hypoxia die or suffer from moderate to severe disabilities such as cerebral palsy or developmental delays by 18 to 22 months of age. According to published results, the incidence of asphyxia increases with natural childbirth, and the highest rates are currently seen in the provinces of Kurdistan, Razavi Khorasan, and Sistan and Baluchestan. However, only a handful of hospitals in Iran, including those in Tehran, Mashhad, and a few other provincial centers, have neonatal cooling devices available and operational.
Report on the Incidence of Asphyxia in Iran
In a report titled “Asphyxia in Iran” published on the Aparat, Neonatal Health channel, Dr. Heidarzadeh, a neonatology specialist, provided statistics on asphyxia in Iran.
During this presentation, which pertains to October 2021, data related to asphyxia from 2018 to spring 2021 were reviewed. Here are some of the key points:
Interested individuals can view the full report via the link below.
Asphyxia in Iran – Neonatal Health – Aparat
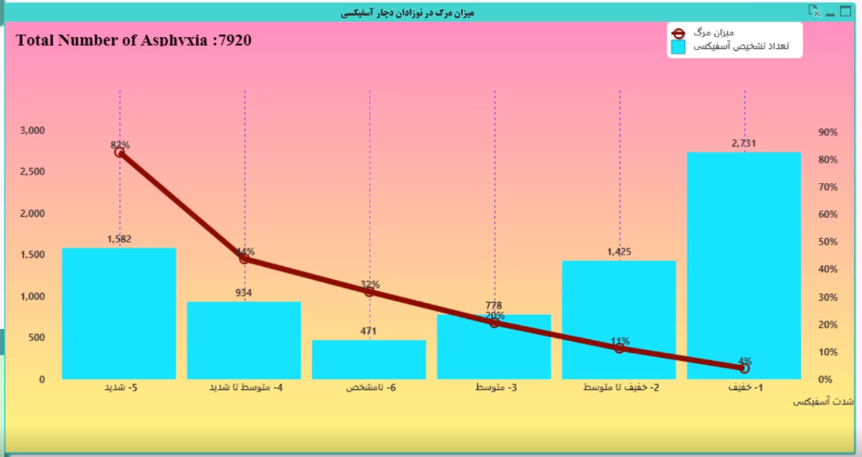
The total number of asphyxia cases in Iran from 2018 to spring 2021, categorized by severity, is as follows: a total of 7,920 cases were reported, including 2,731 mild cases, 1,425 mild to moderate cases, 778 moderate cases, 934 moderate to severe cases, 1,100 severe cases, and 471 unspecified cases.
In this report, the mortality rate for infants with severe asphyxia was 82%, and for those with moderate to severe asphyxia, it was 44%.
The presentation also included a report on the hospitalization rate of infants due to asphyxia and the trend of cooling therapy in asphyxiated infants. Additionally, the relationship between the type of delivery and the incidence of asphyxia was examined. According to the report, the provinces of Kurdistan, Razavi Khorasan, Sistan and Baluchestan, Khuzestan, Hormozgan, Kerman, and Kermanshah have the highest rates of asphyxia per 1,000 live births in the country.
For complete details of this report, you can visit the link below.
Asphyxia in Iran – Neonatal Health – Aparat